
Administered via the pulmonary route, INBRIJA
complements oral CD/LD treatment21
Avoids absorption variability
caused by the GI tract3
Well suited for on-demand use.21
See dosing information
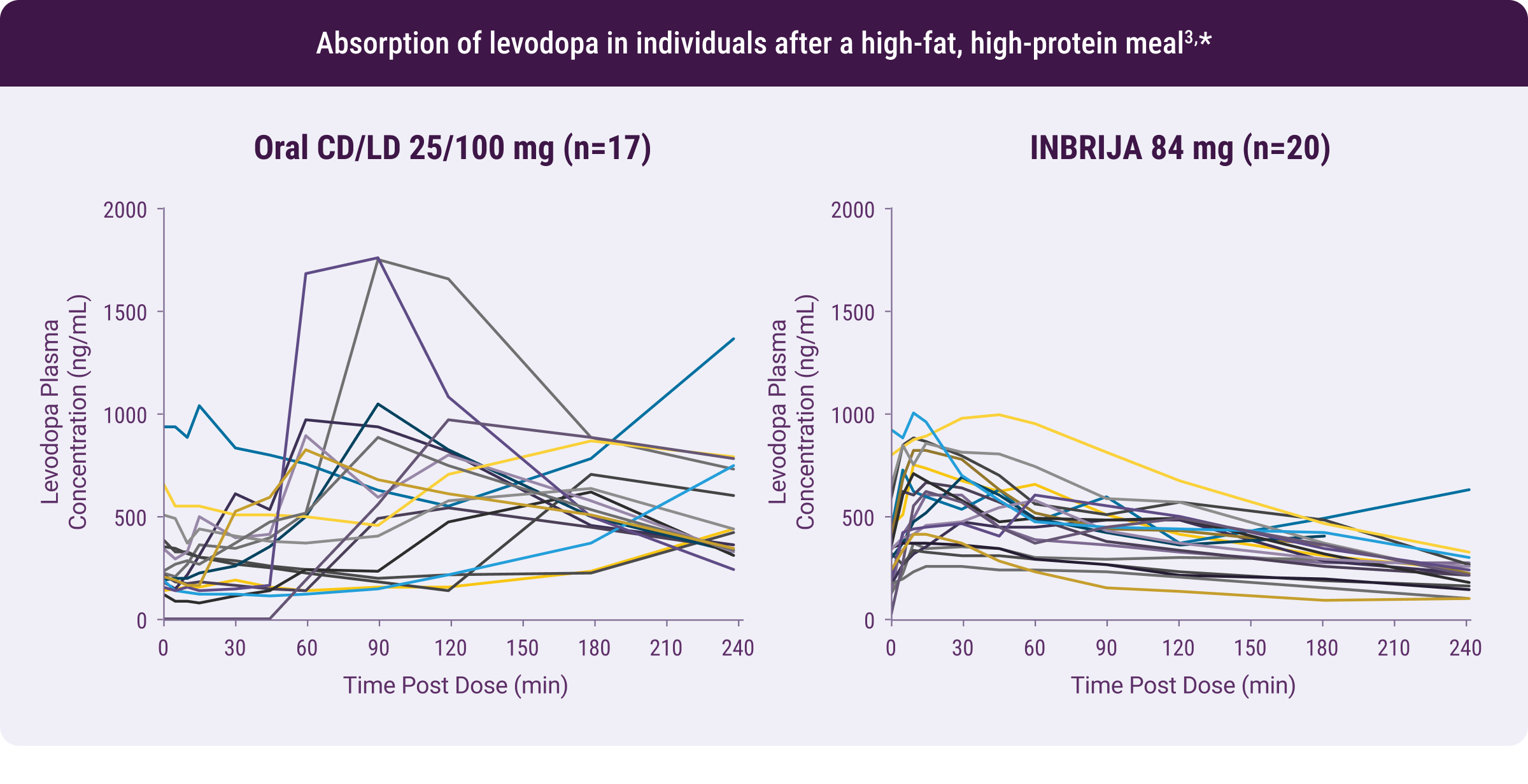
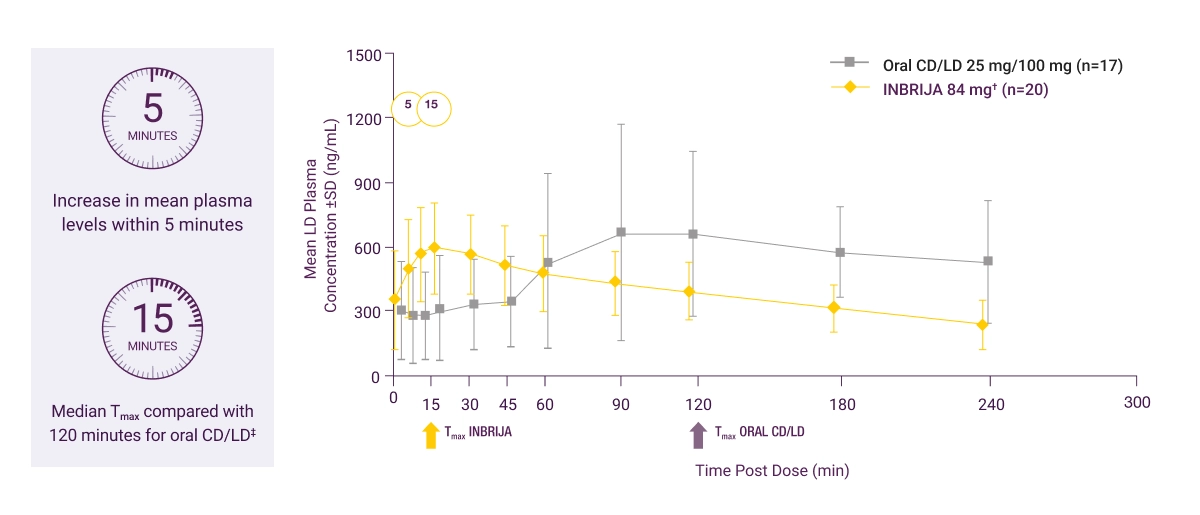
Patterns of plasma absorption of oral CD/LD and inhaled levodopa3,*
Patterns of plasma absorption of oral CD/LD and inhaled levodopa3,*
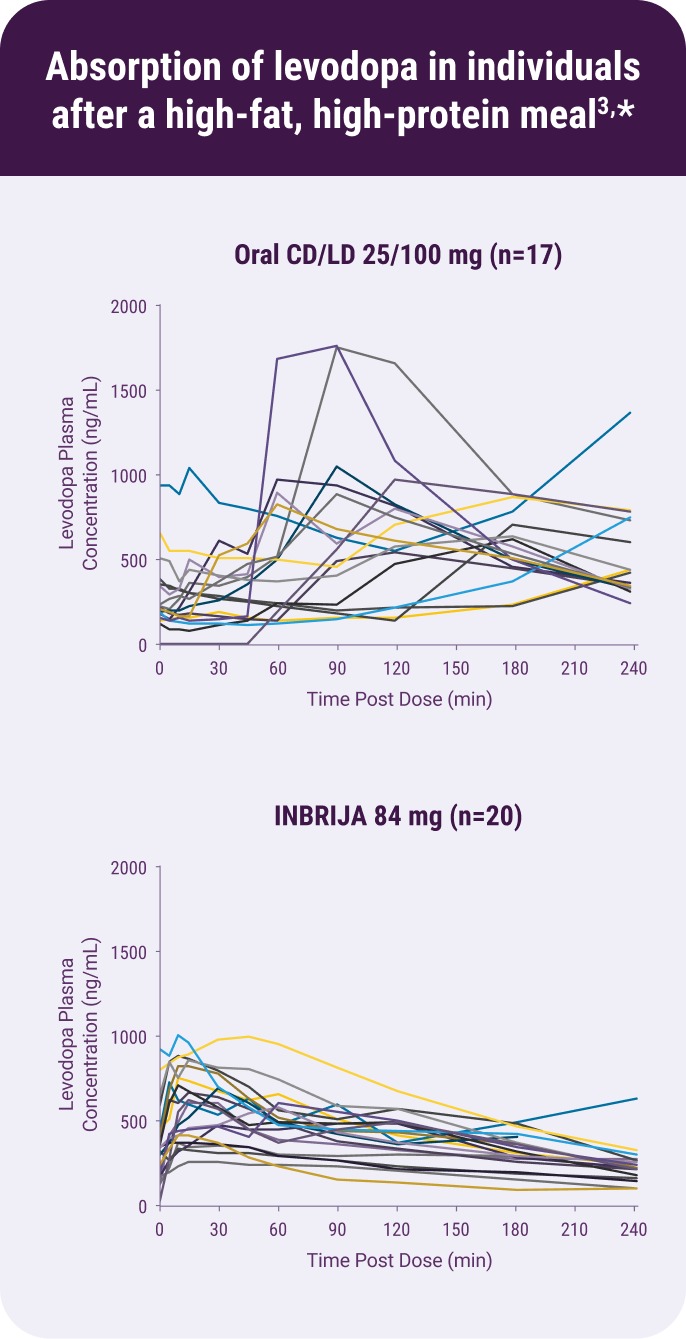
Results from a randomized, open-label, 2-way crossover study evaluating the pharmacokinetics of a single inhaled dose of INBRIJA 84 mg, administered with oral carbidopa 25 mg, and a single ingested dose of CD/LD 25/100 mg in fed state in patients with PD who were regularly taking oral CD/LD.3
Mean LD plasma concentrations after a dose of INBRIJA 84 mg or oral CD/LD 25/100 mg following a high-fat, high-protein meal3,*
* |
4 to 5 hours after morning CD/LD, patients ate a meal and then received study drug. No clinical conclusions can be drawn from this PK study.3 |
† |
INBRIJA 84 mg coadministered with 25 mg oral carbidopa for true pharmacokinetic comparison to levodopa.3 |
‡ |
Median Tmax represented to account more accurately for outliers. |
|
CD/LD, carbidopa/levodopa; GI, gastrointestinal; PD, Parkinson's disease; SD, standard deviation; Tmax, time to peak drug concentration. |
Dr Falconer Video Series:
In Which Patients Should
On-Demand Therapy Be
Considered as a Treatment Option?
Dr Falconer is a board-certified neurologist and a trained movement specialist who works in the advanced care of patients with Parkinson's disease.

