
INBRIJA®—the only inhaled levodopa for on-demand use in patients taking CD/LD.21
Here are 2 ways to prescribe INBRIJA*:
ePrescribe INBRIJA in 2 simple steps
1-949-524-3566
(Recommended)
NCPDP: 5664417
NPI: 1871002485
Address:
361 Hospital Rd., Ste 425
Newport Beach, CA 92663
 print instructions
print instructions

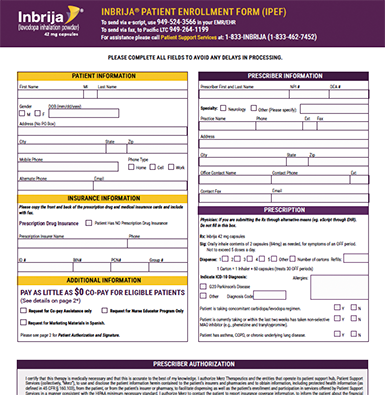
Complete the Patient Enrollment Form
(Formerly known as Prescription Request Form)
FILL OUT FORM
Download and fill out a Patient Enrollment Form
FAX
Fax completed form to 1-949-264-1199
If you do not have access to a fax machine, call us at 1-833-INBRIJA (1-833-462-7452).
* |
Available at a variety of specialty pharmacies nationwide. |
† |
You may receive a phone call from an INBRIJA patient support specialist if additional information is required to initiate prior authorization. |
‡ |
Standard text and data rates may apply. |
|
EMR, electronic medical record. |
INBRIJA prescription and patient support
INBRIJA prescription process
Submit eRx or Patient Enrollment Form (iPEF)
To Pacific LTC Pharmacy via e-script, use 1-949-524-3566 in your EMR/EHR
Patient support services
Benefits Investigation, Prior Authorization, and Appeals Support
Savings and Financial Assistance Eligibility Determined
Nurse Educator Inhaler Training and Support
Specialty§ pharmacy
Patient
§ |
Available at a variety of specialty pharmacies nationwide. |
|
EHR, electronic health record. |