The levodopa therapeutic window narrows as disease progresses, increasingly resulting in motor fluctuation despite best therapeutic efforts6
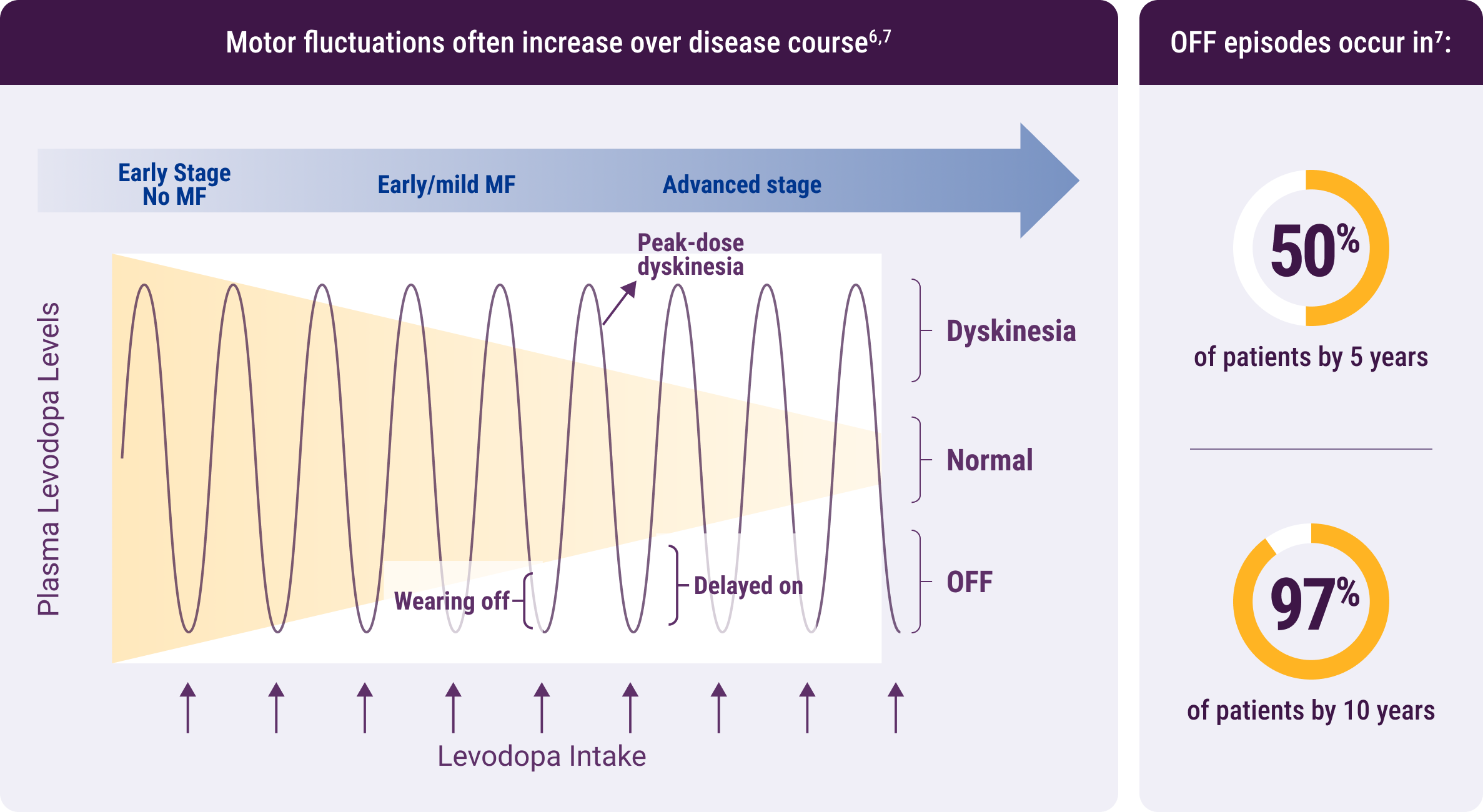
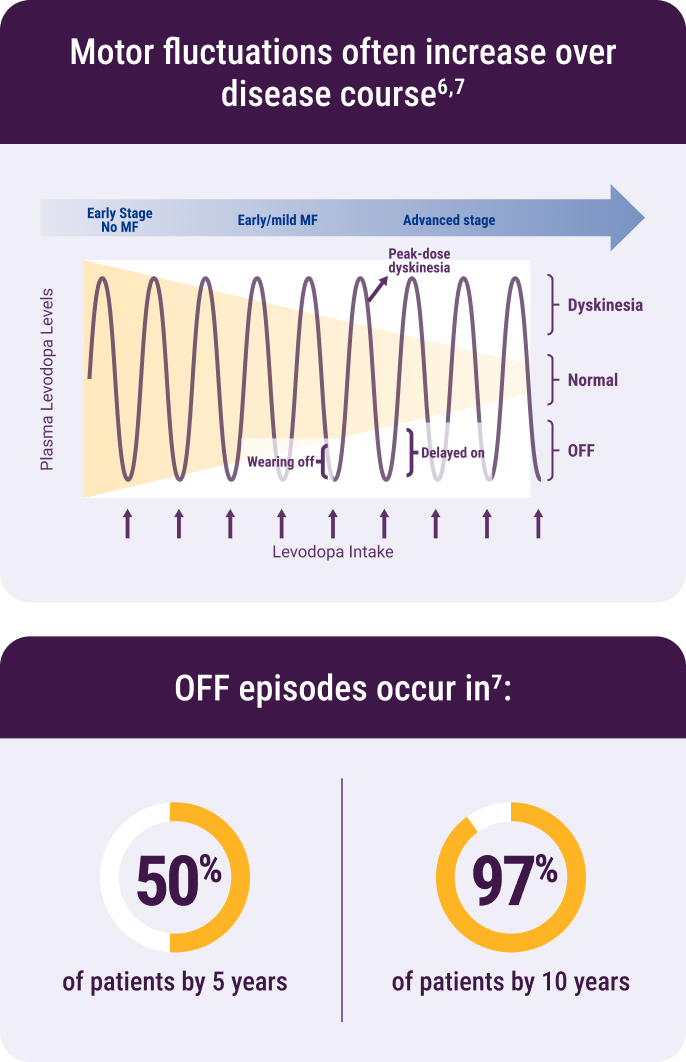
MF, motor fluctuations.
53%
of patients don't always discuss return of motor symptoms with their doctors, despite increasing motor fluctuations8
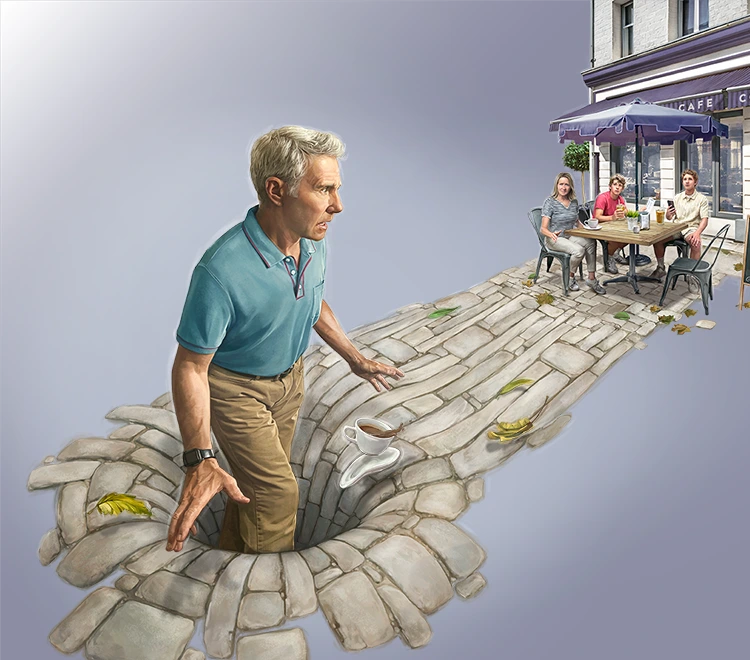
Patients report many ways that motor-symptom return alters their lives9-13,*:

Difficulty getting around due to poor
balance or freezing of gait

Not wanting to go to restaurants due to
difficulty handling utensils

Avoiding being seen in public due to
tremor or bradykinesia

Fearing falling in public due to postural
instability or poor balance
Based on statistically significant associations with OFF periods shown in a cross-sectional survey of 722 patients with Parkinson's disease (PD).
Dr Falconer Video Series:
On-Demand Therapy: Changing the Treatment Paradigm in PD
Dr Falconer is a board-certified neurologist and a trained movement specialist who works in the advanced care of patients with Parkinson's disease.

The first time I realized that my hand was shaking, I decided not to go to work because I was embarrassed.
– Real patient with PD12
OFF periods have a way of shrinking your world.
– Real patient with PD