
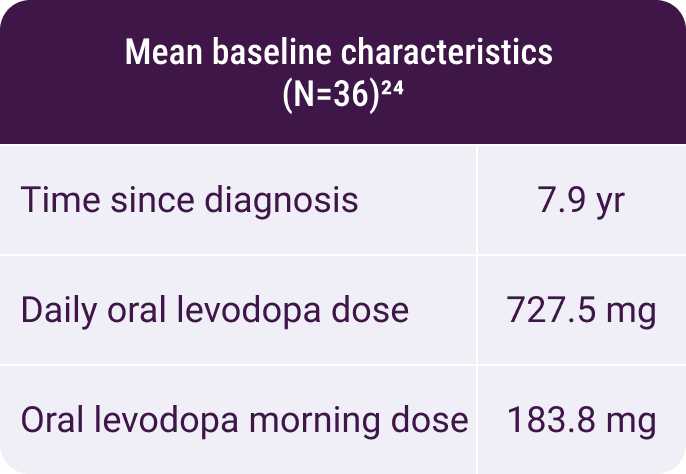
In a randomized, placebo-controlled study using INBRIJA during morning OFF episodes,
no additional safety concerns were reported24
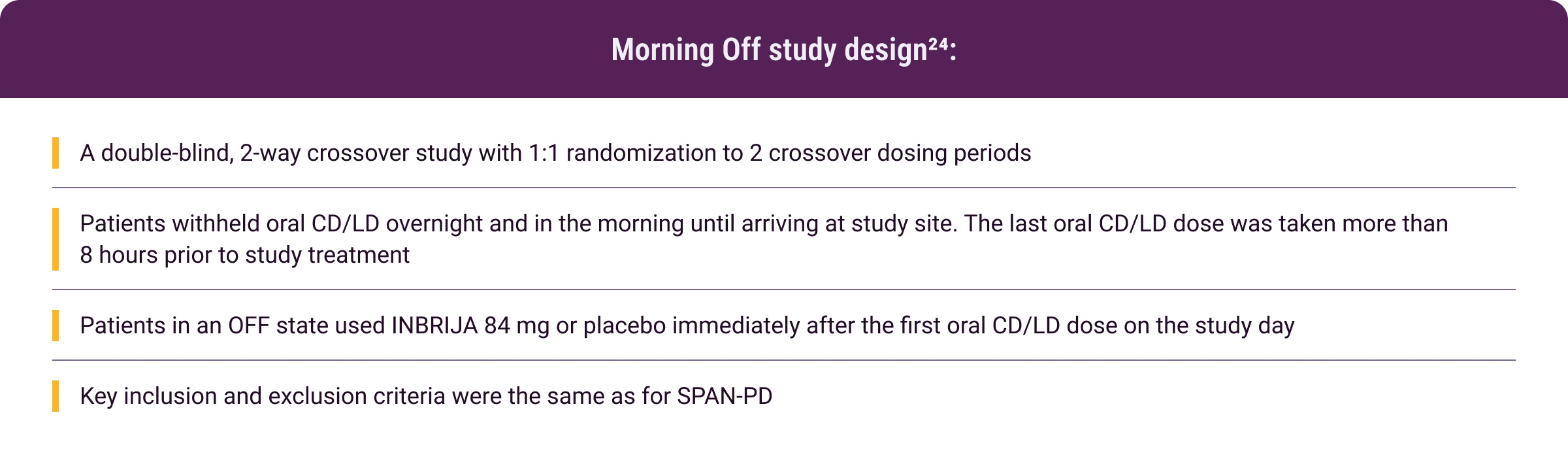
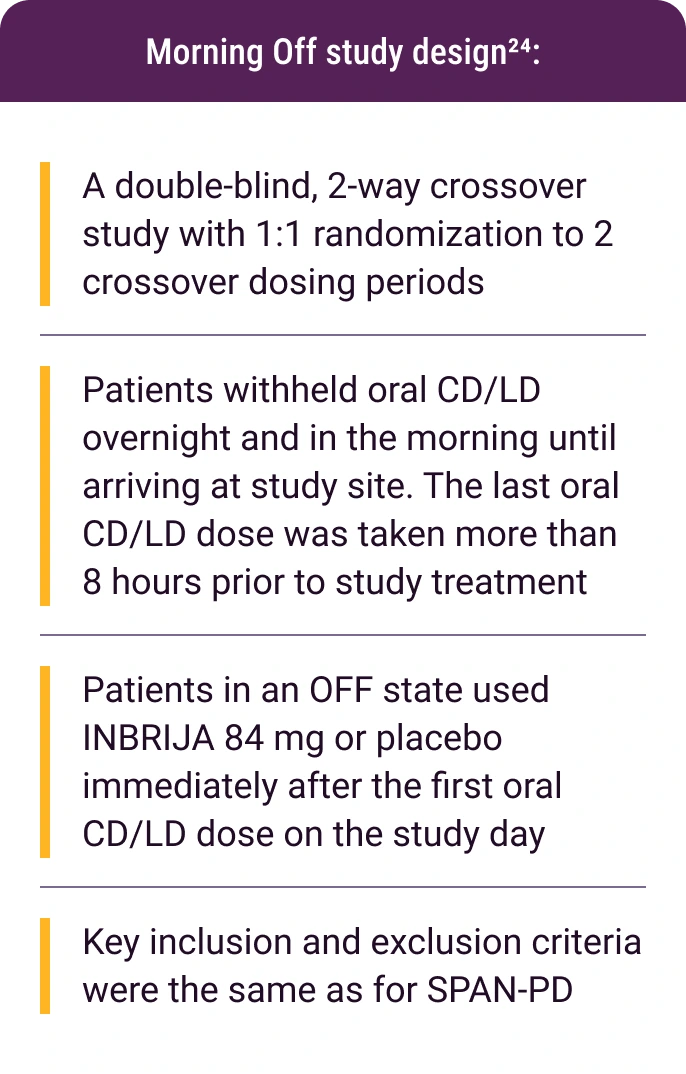
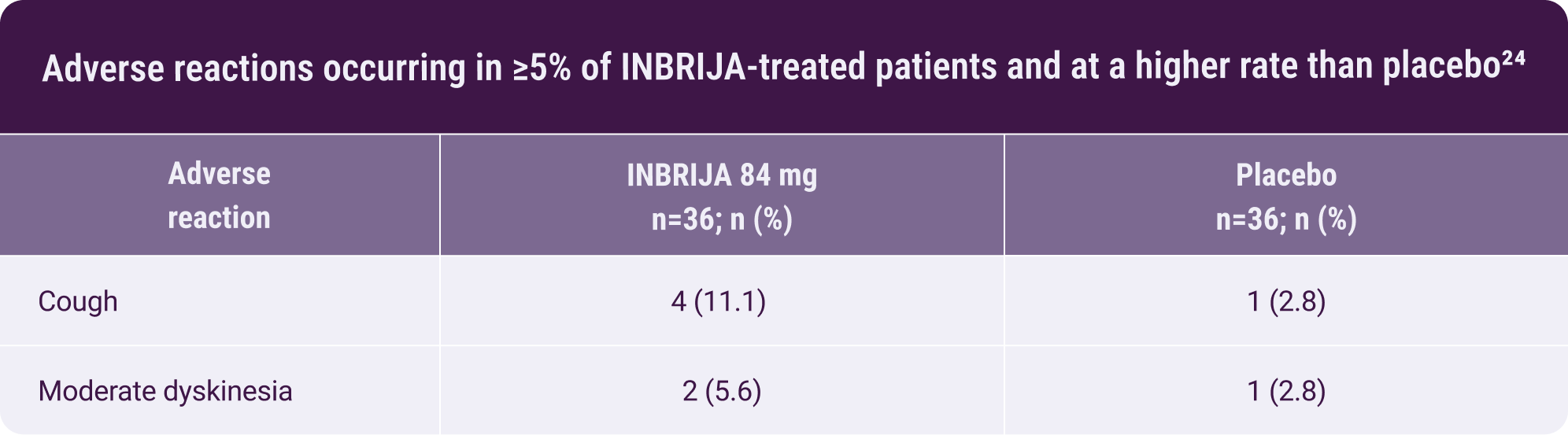
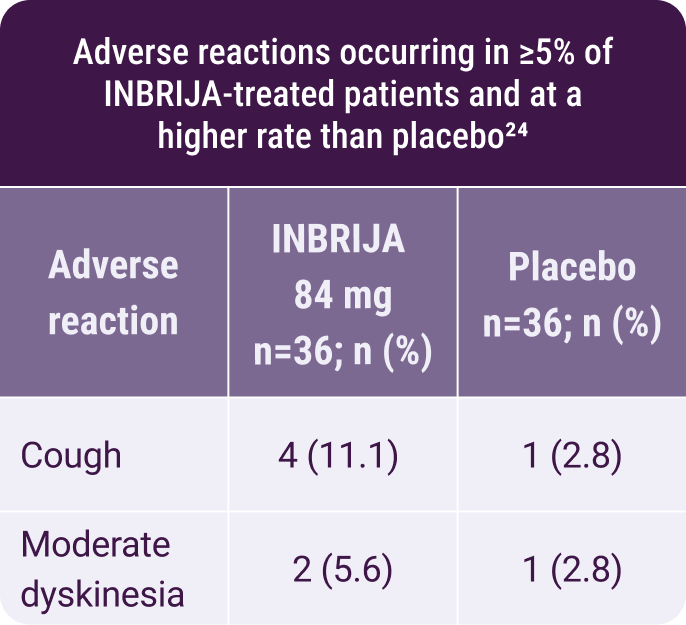
- There were no discontinuations due to adverse reactions24
In a randomized, placebo-controlled study using INBRIJA during
morning OFF episodes24:
Moderate dyskinesia was reported in
2 of 36 patients treated with INBRIJA
No additional safety
concerns
were reported
CD/LD, carbidopa/levodopa.